Post mastectomy pain syndrome (PMPS) is a chronic pain condition that affects many breast cancer survivors. While often confused with phantom breast pain or complex regional pain syndrome, PMPS has distinct nerve-related causes and a serious impact on quality of life.

What Causes PMPS?
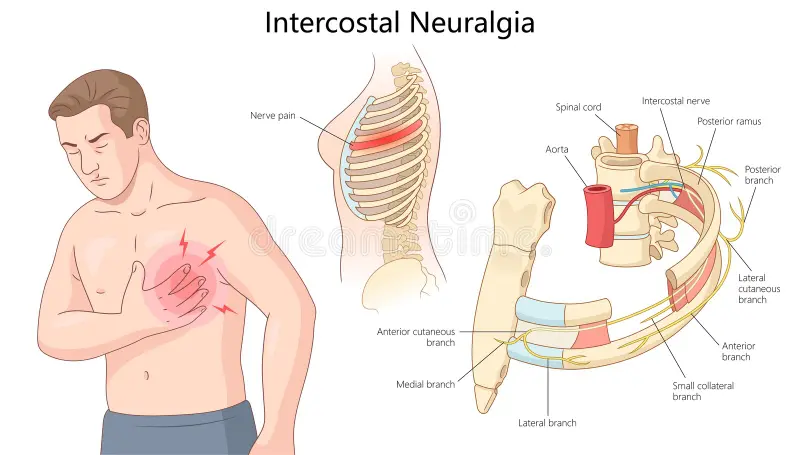
PMPS usually begins with nerve injury during breast surgery—even with careful surgical techniques, some degree of nerve trauma is often unavoidable. The intercostobrachial nerve is frequently affected, especially during lymph node removal. Other nerves, such as the pectoral, thoracodorsal, or long thoracic nerves, can also be involved. These injuries may cause long-term burning, stabbing, or electric-like pain.
Other contributing factors include:
- Radiation therapy, which can scar and inflame tissues
- Chemotherapy, particularly drugs that cause peripheral neuropathy
- Muscle injury, from surgery involving the chest or shoulder
Why Do Ribs Hurt Years After Mastectomy?
Rib pain years after a mastectomy is more common than many realize—and it’s not just a lingering discomfort. It’s often a sign of PMPS, and the pain can be persistent, frustrating, and deeply disruptive.
One of the most common causes is nerve damage. You can read more about this issue in our related article, Breast Cancer and Rib Pain: Causes and How to Find Relief. Nerves around the chest wall—especially the intercostal nerves—can be stretched, cut, or irritated during surgery or radiation. Over time, this may lead to neuroma formation, with tangled, painful nerve endings that generate spontaneous pain signals.
Radiation treatment can also contribute to rib pain. Learn more in our article on managing pain from radiation therapy side effects. Radiation causes tissue fibrosis—scarring and thickening of muscles and nerves in the chest wall. This tight, inflexible tissue may compress nerves or make them hypersensitive.
Some patients also develop central sensitization. This condition makes the nervous system overly responsive, so even gentle touch or normal movements can trigger pain. This explains why rib pain may persist years after surgery.
The pain may be sharp or dull, aching or electric. It might feel like a tight band around the ribs or a jolt with each deep breath. For many, it’s not just physical—it’s a constant reminder of everything they’ve been through.
If you’re experiencing rib pain long after a mastectomy, it’s not all in your head. It doesn’t mean cancer has returned. It means your nerves are still reacting—and you deserve relief.
Who’s at Risk?
You may be more likely to develop PMPS if you:
- Are younger
- Had severe pain immediately after surgery
- Have a history of chronic pain or anxiety
- Received radiation or underwent extensive surgery
How Is PMPS Diagnosed?
There’s no single test for PMPS. Doctors rely on medical history and symptom patterns. To meet the criteria, the pain:
- Begins after breast surgery
- Lasts for at least 3 to 6 months
- Affects the chest, armpit, or upper arm
- Feels burning, stabbing, or electric in nature
It differs from phantom breast syndrome, where pain is felt in a breast that’s no longer present. It also contrasts with CRPS, which causes changes in skin color, swelling, and temperature, usually in a limb.
Real Stories, Real Struggles
Many patients report feeling dismissed when they mention rib or chest pain months or even years after surgery. “I thought I was going crazy,” one woman shared. “Everyone kept telling me it was in my head.”
The emotional toll is real. Recognizing and treating PMPS early can make a profound difference.
Common Myths About Rib Pain After Mastectomy
A common misconception is that rib pain years later must mean cancer has returned. In most cases, it doesn’t. PMPS is a nerve condition—not a recurrence of breast cancer. But it’s still real, and it deserves medical attention.
Delayed Diagnosis Happens Too Often
PMPS is frequently misdiagnosed or completely overlooked. It may be mistaken for muscle strain, scar tissue pain, or even anxiety. Patients can go years without a proper explanation. And the longer it goes untreated, the harder it becomes to manage.
Treatment Options That Work
Managing PMPS requires a step-by-step, personalized approach. Here’s what helps:
Physical Therapy
Targeted exercises and myofascial release can improve movement and ease pain. Studies show physical therapy enhances both quality of life and pain levels.
Electroanalgesia
This non-invasive therapy uses low-level electrical currents to interrupt pain signals. It’s safe, accessible, and especially useful for patients seeking non-drug options.
Medications
Doctors may recommend medications for nerve pain, including:
- Gabapentin or pregabalin
- Amitriptyline
- SSRIs like sertraline
- Topical capsaicin cream
These options can help, but they sometimes cause side effects and should be monitored.
Injections and Nerve Blocks
For localized, stubborn pain, injections may help. These include:
- Intercostobrachial or paravertebral nerve blocks
- Botulinum toxin injections
- Pulsed radiofrequency therapy
In some cases, spinal cord stimulation (SCS) is explored for long-term relief.
Advanced Neuromodulation Options
Spinal cord stimulation (SCS) and peripheral nerve stimulation (PNS) offer promising relief for patients with severe or resistant PMPS.
Spinal Cord Stimulation (SCS):
SCS delivers gentle electrical pulses to the spinal cord, disrupting pain signals. After a successful trial run, the system can be implanted. Patients often experience a meaningful improvement in mobility, sleep, and mood.
Peripheral Nerve Stimulation (PNS):
PNS targets specific injured nerves. Tiny leads placed near these nerves deliver precise electrical stimulation. It’s minimally invasive and a great option when pain is limited to a specific area.
Both approaches are reversible and well-tolerated in the right candidates.
Mind-Body Therapies
Cognitive-behavioral therapy (CBT) and stress-reduction strategies can reduce pain intensity and help patients regain control. Integrating psychological care into pain management leads to better outcomes.
Why PMPS Matters in Cancer Survivorship
PMPS can disrupt sleep, limit daily activities, and take an emotional toll. For cancer survivors, it can feel like the healing process is never truly complete. Recognizing and treating PMPS is essential to full recovery—not just physically, but emotionally.
Can PMPS Be Prevented?
Yes, in many cases. These steps help reduce the risk:
- Using nerve blocks during surgery
- Administering lidocaine infusions during and after surgery
- Choosing surgical techniques that preserve nerve pathways
Let’s Wrap It Up
Post mastectomy pain syndrome is real—and often misunderstood. Rib pain years after surgery doesn’t mean you’re imagining things. It means your nerves may still be healing. And healing requires help.
Ready to Feel Better?
If you’ve been silently struggling, now is the time to take action. At Red Butte Pain Solutions, we’re here to help. If you’re dealing with post mastectomy pain syndrome or rib pain years after mastectomy, our team is ready.
We proudly care for patients in Tempe, Maricopa, Casa Grande, Gilbert, Sun Lakes, Laveen, Mesa, and Ahwatukee.
Schedule now or call 602-633-4334. Relief is possible.